IMPORTANCE Pigmented lesions in decorative tattoos cause
diagnostic difficulties at a clinical and dermoscopic level. In cases of laser
removal of tattoos, hidden suspicious nevi may be revealed gradually.
OBSERVATIONS We describe the first case of a malignant
melanoma that developed on a preexisting nevus within a tattoo during and
between the phases of laser removal. The patient refused to undergo excision of
the nevus until we made excision conditional for continued laser treatment.
CONCLUSIONS AND RELEVANCE The English literature reports 16
cases of malignant melanoma developing in tattoos. Correlation between the
placement of tattoos and the development of malignant melanoma remains unclear.
Our case emphasizes the diagnostic problems of pigmented lesions within
tattoos. For safety reasons, tattoos should never be placed on pigmented
lesions; if they are, the tattoos should not undergo laser treatment. We
suggest an excision before starting laser tattoo removal. Dermoscopic
assessments on a regular basis during the period of tattoo removal are
recommended. JAMA Dermatol. 2013;149(9):1087−1089.
doi:10.1001/jamadermatol.2013.4901 Published online July 31, 2013
The number of decorative tattoos has been increasing, as has the demand for
their removal by laser devices. Traumatic events, such as UV and ionizing
radiation, mechanical trauma, persistent inflammatory reactions, and burning,
have been discussed as cofactors for neoplasm.1,2 Only 16 cases in
the English literature document malignant melanoma developing in
tattoos.3−5 We herein describe a malignant melanoma that developed
on a nevus within a tattoo that had undergone removal by laser.
Report of a Case A white man aged 29 years presented to our clinic for the
first time in 2001 to have his decorative tattoos removed by laser. The large
multicolored tattoos on both arms and his chest had been applied approximately
10 years earlier (Figure 1). After detailed informed consent, we started tattoo
removal in March of 2002 using a Q-switched Nd:YAG laser (Affinity QS;
Cynosure) set to a wavelength of 1064 nm to treat black ink and 532 nm to treat
red and orange dye. We started with 1.0 J/cm2 , and in the course of the
treatment we increased energy up to 7.1 J/cm2 for the 1064−nm wavelength (spot
size, 4 mm) and 1.5 J/cm2 for the 532−nm wavelength (spot size, 6 mm).
 Owing to
the extreme size of the tattoo, only partial treatment could be applied during
each session. Because of a loss of response after 43 sessions, we started using
a Q-switched alexandrite laser (Accolade; Cynosure). The energy was increased
from 4.0 to 4.8 J/cm2 with a spot size of 4 mm. Before laser treatment, we
assessed the patient’s skin and noticed a nevus on his right shoulder. Because
the nevus was situated within the laser area, we strongly advised him to have
it excised. Possible changes within the nevus were barely detectable because of
the intracutaneous black tattoo pigments in the area. Initial dermoscopy
findings showed no atypical signs. The patient strictly refused exc ision. We
repeated our explic it request for him to have this nevus removed several
times, and he rejected each request. In November of 2009, after a total of 47
laser sessions, we informed the patient that we would not continue laser
treatment because of forensic reasons, and he agreed to have the nevus excised
(Figure 2). At that time, dermoscopy findings showed characteristics of an
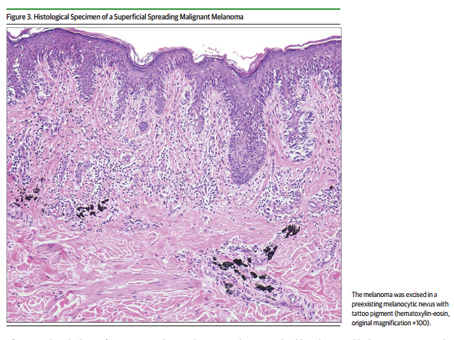
early melanoma. The excisional biopsy results showed the lesion to be a Clark
level II superficial spreading malignant melanoma with a Breslow thickness of
0.45 mm (Figure 3). Chest radiography and lymph node ultrasonography yielded no
abnormalities. The patient refused a second excision with a free margin.
Owing to
the extreme size of the tattoo, only partial treatment could be applied during
each session. Because of a loss of response after 43 sessions, we started using
a Q-switched alexandrite laser (Accolade; Cynosure). The energy was increased
from 4.0 to 4.8 J/cm2 with a spot size of 4 mm. Before laser treatment, we
assessed the patient’s skin and noticed a nevus on his right shoulder. Because
the nevus was situated within the laser area, we strongly advised him to have
it excised. Possible changes within the nevus were barely detectable because of
the intracutaneous black tattoo pigments in the area. Initial dermoscopy
findings showed no atypical signs. The patient strictly refused exc ision. We
repeated our explic it request for him to have this nevus removed several
times, and he rejected each request. In November of 2009, after a total of 47
laser sessions, we informed the patient that we would not continue laser
treatment because of forensic reasons, and he agreed to have the nevus excised
(Figure 2). At that time, dermoscopy findings showed characteristics of an
early melanoma. The excisional biopsy results showed the lesion to be a Clark
level II superficial spreading malignant melanoma with a Breslow thickness of
0.45 mm (Figure 3). Chest radiography and lymph node ultrasonography yielded no
abnormalities. The patient refused a second excision with a free margin.
 Discussion Before laser tattoo removal, skin should be examined as
thoroughly as possible for hidden pigmented lesions. In cases of nonadherence
to medical advice (as discussed herein), laser treatment should be withheld
until the recommended excision has taken place. Suspicious nevi can be covered
by tattoos, and assessing the nevi is extremely difficult at the clinical and
dermoscopic levels.6 Tattooing also causes difficulties in assessing a sentinel
lymph node biopsy specimen because the pigment can mimic metastatic disease and
thus provide a challenge for surgeons and pathologists.7 We
recommend dermoscopic assessments on a regular basis while a tattoo is
undergoing removal by laser. For this reason, laser removal of tattoos should
be performed by dermatologists and not by nonprofessionals.8
Discussion Before laser tattoo removal, skin should be examined as
thoroughly as possible for hidden pigmented lesions. In cases of nonadherence
to medical advice (as discussed herein), laser treatment should be withheld
until the recommended excision has taken place. Suspicious nevi can be covered
by tattoos, and assessing the nevi is extremely difficult at the clinical and
dermoscopic levels.6 Tattooing also causes difficulties in assessing a sentinel
lymph node biopsy specimen because the pigment can mimic metastatic disease and
thus provide a challenge for surgeons and pathologists.7 We
recommend dermoscopic assessments on a regular basis while a tattoo is
undergoing removal by laser. For this reason, laser removal of tattoos should
be performed by dermatologists and not by nonprofessionals.8
Pigmented lesions should not be treated by laser because of forensic
considerations and to prevent potential laserinduced changes. In 2004, Kerl et
al9 published a tale of caution concerning laser therapy and melanocytic nevi
and emphasized that, for most melanocytic lesions, laser therapy is not
appropriate.9 No scientific evidence suggests that laser treatment
converts benign nevi into melanoma, and we will never know if the nevus in our
case would have progressed the same way with or without laser treatment. In the
course of Q-switched laser treatment, pigmented cells can lose pigmentation,
thus making assessment of melanocytic lesions more difficult.
Kopera et al10 already described the pitfalls of treating
melanocytic lesions by laser: S-100–positive cells persisted ex vivo throughout
a single course of Q-switched ruby laser exposure. In 2000, Kaskel et
al11evaluated the relationship between traumatic events (eg, applying or
removing a tattoo) and melanoma characteristics by means of a retrospective
questionnaire addressed to 369 patients with melanoma. The authors found no
evidence that traumatic events are a causative factor for melanoma
formation.11 Tattoo removal with laser therapy also releases
potentially toxic substances, such as dibutyl phthalate in black ink, with
unknown long-term consequences.5,12 Gottschaller et al13
presume that the main danger of treating a pigmented lesion by laser is a
clinical misdiagnosis, whether the lesion was a primary malignant melanoma or
whether a malignant melanoma was induced by the laser treatment. In 2010,
Zipser et al14discussed the outcomes of 12 patients
presentingwithmelanoma subsequent to previous treatment with laser.
They found that treating pigmented lesions with a laser delays the diagnosis
of melanoma and thus prevents the timely beginning of the necessary therapy.
The authors suggest that laser treatment of melanocytic nevi is often based on
a clinical or histological misdiagnosis and that more unreported cases exist.
They also raise the question of the possibility of melanoma induction by laser.
Lee and Busam15 emphasize the importance of dermoscopy and, if
necessary, performing appropriate biopsies before laser treatment. With these
aspects in mind, we would make a different decision in the future and exclude
pigmented lesions within tattoos from laser treatment in general. In the
present case, we want to emphasize the diagnostic problems of pigmented lesions
within tattoos and the danger
 ARTICLE INFORMATION Accepted for Publication: April 4, 2013.
Published Online: July 31, 2013. doi:10.1001/jamadermatol.2013.4901. Author
Contributions: All authors had full access to all the data in the study and
take responsibility for the integrity of the data and the accuracy of the data
analysis. Study concept and design: All authors. Acquisition of data: Pohl.
Analysis and interpretation of data: Raulin. Drafting of the manuscript: Pohl.
Critical revision of the manuscript for important intellectual content: All
authors. Statistical analysis: Raulin. Administrative, technical, or material
support: All authors. Study supervision: Raulin. Conflict of Interest
Disclosures: None reported. Additional Contributions: Markus Hantschke, MD,
Dermatopathologie Friedrichshafen, Germany, provided the image used in Figure
3.
ARTICLE INFORMATION Accepted for Publication: April 4, 2013.
Published Online: July 31, 2013. doi:10.1001/jamadermatol.2013.4901. Author
Contributions: All authors had full access to all the data in the study and
take responsibility for the integrity of the data and the accuracy of the data
analysis. Study concept and design: All authors. Acquisition of data: Pohl.
Analysis and interpretation of data: Raulin. Drafting of the manuscript: Pohl.
Critical revision of the manuscript for important intellectual content: All
authors. Statistical analysis: Raulin. Administrative, technical, or material
support: All authors. Study supervision: Raulin. Conflict of Interest
Disclosures: None reported. Additional Contributions: Markus Hantschke, MD,
Dermatopathologie Friedrichshafen, Germany, provided the image used in Figure
3.
REFERENCES
-
Khan IU, Moiemen NS, Firth J, Frame JD. Malignant melanoma
disguised by a tattoo [case report]. Br J Plast Surg. 1999;52(7):598.
-
Kluger N, Phan A, Debarbieux S, Balme B, Thomas L. Skin
cancers arising in tattoos: coincidental or not? Dermatology.
2008;217(3):219−221.
-
Paradisi A, Capizzi R, De Simone C, Fossati B, Proietti I,
Amerio PL. Malignant melanoma in a tattoo: case report and review of the
literature. Melanoma Res. 2006;16(4):375−376.
-
Varga E, Korom I, Varga J, Kohán J, Kemény L, Oláh J.
Melanoma and melanocytic nevi in decorative tattoos: three case reports.J Cutan
Pathol. 2011;38(12):994−998.
-
Kluger N, Koljonen V. Tattoos, inks, and cancer. Lancet
Oncol. 2012;13(4):e161−e168.
-
Gall N, Bröcker EB, Becker JC. Particularities in managing
melanoma patients with tattoos: case report and review of the literature.J
Dtsch Dermatol Ges. 2007;5(12):1120−1121.
-
Singh RS, Hafeez Diwan A, Prieto VG. Potential diagnostic
pitfalls in melanoma arising in a cutaneous tattoo. Histopathology.
2007;51(2):283−285.
-
Karsai S, Krieger G, Raulin C. Tattoo removal by
non-professionals: medical and forensic considerations.J Eur Acad Dermatol
Venereol. 2010;24(7):756−762.
-
Kerl H, Raulin C, Landthaler M. Controversy in dermatology:
laser therapy and melanocytic nevi [in German].J Dtsch Dermatol Ges. 2004;2(8):
681−683.
-
Kopera D, Hohenleutner U, Stolz W, Landthaler M. Ex vivo
quality-switched ruby laser irradiation of cutaneous melanocytic lesions:
persistence of S-100–, HMB-45– and Masson-positive cells. Dermatology.
1997;194(4):344−350.
-
Kaskel P, Kind P, Sander S, Peter RU, Krähn G. Trauma and
melanoma formation: a true association? Br J Dermatol.
2000;143(4):749−753.
-
12. Lehner K, Santarelli F, Vasold R, König B, Landthaler M,
Bäumler W. Black tattoo inks are a source of problematic substances such as
dibutyl phthalate. Contact Dermatitis. 2011;65(4):231−238.
-
Gottschaller C, Hohenleutner U, Landthaler M. Metastasis of a
malignant melanoma 2 years after carbon dioxide laser treatment of a pigmented
lesion: case report and review of the literature. Acta Derm Venereol.
2006;86(1):44−47.
-
Zipser MC, Mangana J, Oberholzer PA, French LE, Dummer R.
Melanoma after laser therapy of pigmented lesions: circumstances and outcome.
Eur J Dermatol. 2010;20(3):334−338. 15. Lee EH, Busam KJ. Desmoplastic melanoma
presenting after laser treatment: a case report and tale of caution. Dermatol
Surg. 2011;37(11):1689−1692.
.jpg)




